
Labor/Delivery

“Maternal & Newborn Health: Labor and Delivery” is a crucial component of the NCLEX-PN® exam. It focuses on the stages of labor, maternal care, fetal monitoring, and managing complications. LPNs play a vital role in supporting mothers during labor, promoting safety, and ensuring positive outcomes. Key topics include labor progression, pain management, fetal heart rate monitoring, and emergency interventions like managing umbilical cord prolapse and uterine rupture. Mastering these concepts is essential for providing safe, effective care to mothers and newborns.
Learning Objectives
In studying “Maternal & Newborn Health: Labor/Delivery” for the NCLEX-PN® Exam, you should learn to understand the stages of labor, focusing on the physiological changes and nursing interventions required at each stage. Analyze the roles and responsibilities of LPNs during labor, delivery, and immediate postpartum care. Evaluate factors affecting labor progression, such as fetal position, maternal status, and labor complications. Explore nursing considerations like fetal heart rate monitoring, pain management, and emergency interventions. Apply knowledge to ensure safe delivery, effective communication, and proper maternal and newborn care. Emphasize emergency response to conditions like prolapsed cord, shoulder dystocia, and uterine rupture.
1. Stages of Labor and Delivery
Labor and delivery are critical phases in the childbirth process. For the NCLEX-PN® exam, it is essential to understand the stages of labor, nursing responsibilities, and the interventions required for a safe delivery. Labor is divided into four distinct stages, each with unique physiological processes and nursing care requirements.
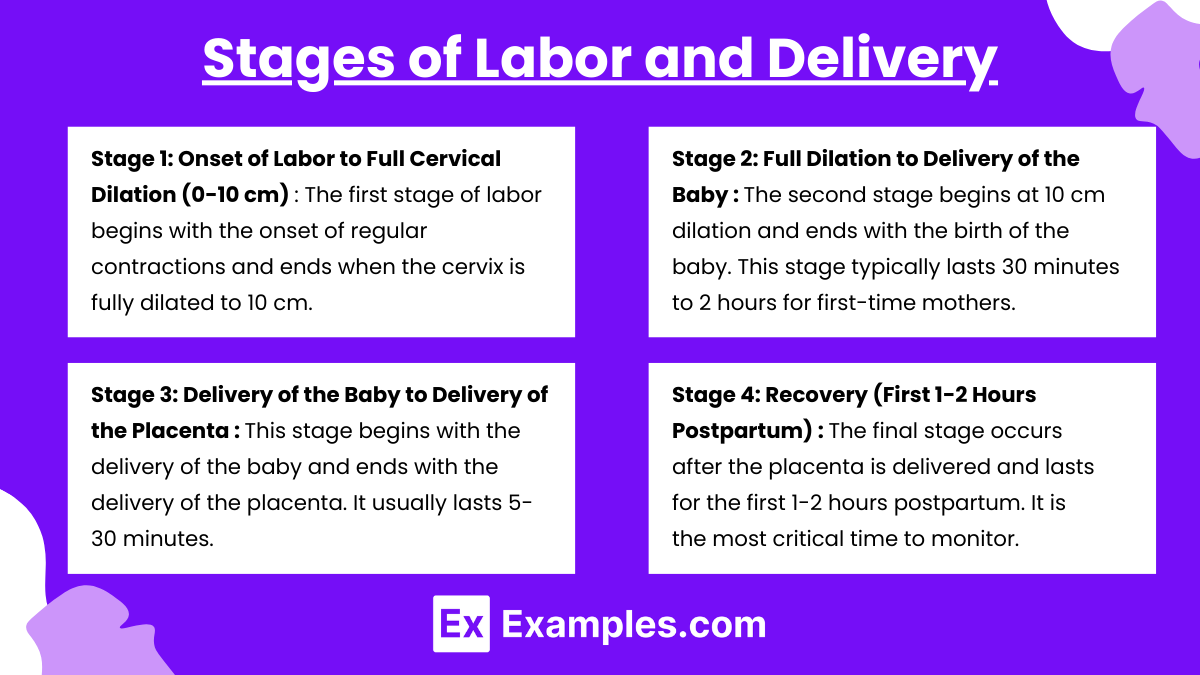
Stage 1: Onset of Labor to Full Cervical Dilation (0-10 cm)
The first stage of labor begins with the onset of regular contractions and ends when the cervix is fully dilated to 10 cm. This stage is the longest stage of labor.
Phases of Stage 1
- Latent Phase (0-3 cm dilation)
- Contractions: Mild, irregular, lasting 30-45 seconds, every 5-30 minutes.
- Maternal Behavior: Excited, talkative, and able to move around.
- Nursing Interventions: Provide comfort, encourage ambulation, and offer relaxation techniques.
- Active Phase (4-7 cm dilation)
- Contractions: Moderate to strong, lasting 40-70 seconds, every 3-5 minutes.
- Maternal Behavior: More focused, quieter, and needs encouragement.
- Nursing Interventions: Position changes, breathing techniques, and monitoring fetal heart rate (FHR) and maternal vital signs.
- Transition Phase (8-10 cm dilation)
- Contractions: Strong, intense, lasting 60-90 seconds, every 2-3 minutes.
- Maternal Behavior: Irritable, restless, and may feel the urge to push.
- Nursing Interventions: Provide emotional support, avoid pushing until full dilation, monitor FHR, and offer breathing guidance.
Stage 2: Full Dilation to Delivery of the Baby
The second stage begins at 10 cm dilation and ends with the birth of the baby. This stage typically lasts 30 minutes to 2 hours for first-time mothers.
Key Events of Stage 2
- Descent and Crowning: The baby’s head becomes visible at the vaginal opening.
- Pushing: The mother actively pushes during contractions to deliver the baby.
- Nursing Interventions:
- Encourage effective pushing (using breath-holding and bearing down techniques).
- Support the mother’s positioning (upright, squatting, or side-lying).
- Monitor Fetal Heart Rate (FHR) continuously for signs of fetal distress (e.g., late decelerations).
Stage 3: Delivery of the Baby to Delivery of the Placenta
This stage begins with the delivery of the baby and ends with the delivery of the placenta. It usually lasts 5-30 minutes.
Key Events of Stage 3
- Placental Separation: Signs include a sudden gush of blood, lengthening of the umbilical cord, and a change in the shape of the uterus.
- Delivery of Placenta: The placenta is expelled with gentle traction on the cord.
- Nursing Interventions:
- Monitor for signs of placental separation.
- Assess for signs of retained placenta, which may cause postpartum hemorrhage.
- Check the placenta for completeness to ensure no retained fragments are left inside the uterus.
Stage 4: Recovery (First 1-2 Hours Postpartum)
The final stage occurs after the placenta is delivered and lasts for the first 1-2 hours postpartum. It is the most critical time to monitor for postpartum hemorrhage.
Key Events of Stage 4
- Maternal Stabilization: The uterus contracts to prevent bleeding.
- Initial Bonding: The mother is encouraged to breastfeed and bond with the baby.
- Nursing Interventions:
- Monitor Fundus: Check for firmness and location. A firm fundus prevents excessive bleeding.
- Check for Lochia: Lochia (postpartum vaginal discharge) should be rubra (red) and moderate.
- Monitor Vital Signs: Watch for signs of hypovolemic shock (increased heart rate, decreased BP).
- Assess for Bladder Distention: Encourage voiding to prevent bladder distention, which may displace the uterus and increase bleeding risk.
2. Fetal Monitoring During Labor
Fetal monitoring ensures that the baby is receiving adequate oxygen during labor. Fetal heart rate (FHR) is the most crucial parameter.
1. Normal Fetal Heart Rate (FHR)
- Normal range: 110-160 bpm.
- Variability: Fluctuations in FHR are a sign of fetal well-being.
2.Types of Fetal Heart Rate Decelerations
- Early Decelerations: Normal; caused by head compression during contractions.
- Variable Decelerations: Caused by umbilical cord compression.
- Late Decelerations: Emergency; caused by uteroplacental insufficiency (baby not getting enough oxygen).
3.Nursing Interventions for Abnormal FHR
- For Variable Decelerations: Reposition the mother (left side-lying).
- For Late Decelerations:
- Reposition the mother (left side).
- Administer oxygen via facemask.
- Increase IV fluids (to increase perfusion).
- Notify the healthcare provider.
3. Common Complications of Labor and Delivery
1.Prolapsed Umbilical Cord
- Definition: The umbilical cord slips below the presenting part of the fetus, cutting off oxygen.
- Nursing Interventions:
- Position the mother in knee-chest or Trendelenburg position.
- Use a sterile gloved hand to lift the presenting part off the cord.
- Call for emergency assistance immediately.
2.Fetal Distress
- Definition: Occurs when the fetus is not receiving sufficient oxygen.
- Signs: Abnormal FHR (e.g., late decelerations), reduced fetal movement, and meconium-stained amniotic fluid.
- Nursing Interventions:
- Reposition the mother (left side).
- Administer oxygen via mask.
- Increase IV fluids and notify the healthcare provider.
3.Shoulder Dystocia
- Definition: The baby’s shoulder gets stuck behind the mother’s pubic bone during delivery.
- Nursing Interventions:
- Use the McRoberts Maneuver (flex mother’s legs up toward her chest).
- Apply suprapubic pressure to dislodge the shoulder.
4.Precipitous Labor
- Definition: Labor lasting less than 3 hours from onset to delivery.
- Risks: Uterine rupture, birth injury, and postpartum hemorrhage.
- Nursing Interventions:
- Remain with the patient.
- Prepare for rapid delivery.
- Ensure emergency equipment is available.
5.Uterine Rupture
- Definition: A tear in the wall of the uterus, usually in a woman with a previous cesarean delivery.
- Signs: Sudden severe abdominal pain, abnormal FHR, and fetal parts palpable in the abdomen.
- Nursing Interventions:
- Notify the provider immediately.
- Prepare for emergency C-section.
Examples
Example 1: Prolonged Labor
Prolonged labor occurs when the process of labor lasts longer than 20 hours for a first-time mother or more than 14 hours for a mother who has previously given birth. This delay can result from weak uterine contractions, improper fetal positioning, or cervical dilation failure. In this scenario, a woman in active labor remains stuck at 5 cm dilation despite strong and regular contractions. The nurse’s role is crucial in this situation. The nurse continuously monitors the fetal heart rate to ensure the baby is not in distress, provides emotional support to the mother, and helps her with position changes to facilitate cervical dilation. If progress is insufficient, the healthcare provider may order the administration of oxytocin (Pitocin) to stimulate contractions. The nurse also prepares for potential interventions, such as assisted delivery with forceps or a cesarean section, if labor does not progress.
Example 2: Shoulder Dystocia
Shoulder dystocia occurs when the baby’s head delivers, but the shoulders get stuck behind the mother’s pubic bone, preventing the baby from fully exiting the birth canal. This is a medical emergency as it can restrict blood and oxygen flow to the baby. In this scenario, the nurse responds immediately by guiding the mother into the McRoberts position, which involves pulling her knees up toward her chest to widen the pelvic outlet. The nurse may also assist in applying suprapubic pressure (pushing just above the pubic bone) to dislodge the baby’s shoulder. During this time, the nurse maintains clear communication with the healthcare provider and team to coordinate efforts. If the baby remains stuck, the provider may use specialized maneuvers or require an emergency cesarean section. The nurse also prepares resuscitation equipment for the baby, as shoulder dystocia increases the risk of neonatal asphyxia.
Example 3: Prolapsed Umbilical Cord
A prolapsed umbilical cord is a life-threatening complication where the cord slips below the presenting fetal part, causing cord compression and restricting blood flow and oxygen supply to the baby. This is an obstetric emergency. In this scenario, after the rupture of membranes, the nurse notices the umbilical cord protruding from the vaginal opening. Immediate intervention is required to prevent oxygen deprivation to the baby. The nurse places the mother in a knee-chest position or Trendelenburg position (head down, feet up) to relieve pressure on the cord. Additionally, the nurse uses a sterile-gloved hand to manually lift the baby’s head off the cord to maintain blood flow. While performing these actions, the nurse calls for emergency assistance and prepares for a possible emergency cesarean section. Continuous monitoring of the fetal heart rate is critical during this time to assess the baby’s oxygenation status.
Example 4: Late Decelerations on Fetal Heart Rate (FHR) Monitor
Late decelerations are one of the most critical signs of fetal distress. They occur when the baby’s heart rate drops after the peak of a uterine contraction and return to baseline after the contraction ends. Late decelerations are caused by uteroplacental insufficiency, meaning the placenta is not providing adequate oxygen to the baby. This scenario involves a laboring mother whose fetal heart rate monitor shows late decelerations with every contraction. The nurse must act quickly to protect fetal well-being. Interventions include repositioning the mother (preferably to the left side) to improve blood flow, administering oxygen via facemask at 10L/min, and increasing IV fluid to improve maternal blood pressure and placental perfusion. The nurse also stops oxytocin (if being administered) and notifies the healthcare provider immediately. Continuous monitoring of the fetal heart rate is required to assess for further changes, and preparations may be made for an emergency delivery if decelerations persist.
Example 5: Precipitous Labor
Precipitous labor occurs when labor and delivery happen in less than 3 hours from the onset of contractions to the birth of the baby. This type of labor is unpredictable and can increase the risk of perineal tears, uterine rupture, fetal distress, and head trauma to the newborn. In this scenario, a woman arrives at the hospital already in advanced labor and delivers her baby within 90 minutes. The nurse must remain calm and act quickly, as there may be limited time for provider intervention. The nurse prepares emergency delivery equipment and remains at the mother’s bedside to assist with controlled breathing and pushing. To prevent perineal tearing, the nurse supports the baby’s head during crowning and encourages the mother to slow her pushing efforts. Following delivery, the nurse performs a rapid newborn assessment using the APGAR score and monitors the mother for signs of postpartum hemorrhage. Since the mother’s uterus may not contract properly after rapid labor, the nurse must be vigilant for signs of excessive bleeding.
Practice Questions
Question 1
A nurse is monitoring a laboring client in the transition phase of the first stage of labor. Which of the following signs indicates that the patient is in this phase?
A. Cervical dilation of 3 cm, mild contractions every 10-15 minutes
B. Cervical dilation of 8 cm, strong contractions every 2-3 minutes lasting 60-90 seconds
C. Cervical dilation of 5 cm, moderate contractions every 4-6 minutes lasting 30-45 seconds
D. Cervical dilation of 10 cm, urge to push, and crowning of the fetal head
Answer: B. Cervical dilation of 8 cm, strong contractions every 2-3 minutes lasting 60-90 seconds
Explanation: The transition phase is the final phase of the first stage of labor, marked by cervical dilation from 8 to 10 cm. Contractions become strong, intense, and frequent (every 2-3 minutes) and last 60-90 seconds. The mother often feels irritable, restless, and may experience nausea or the urge to push.
- Option A describes the latent phase (0-3 cm dilation) with mild, irregular contractions.
- Option C describes the active phase (4-7 cm dilation) with moderate contractions.
- Option D indicates the start of the second stage of labor, where the cervix is fully dilated (10 cm) and the baby is ready to be delivered.
Question 2
A nurse is caring for a laboring client. The fetal heart rate (FHR) shows late decelerations on the monitor. Which of the following actions should the nurse take first?
A. Reposition the mother to a left side-lying position
B. Administer oxygen via a face mask at 10 L/min
C. Increase the infusion rate of intravenous fluids
D. Notify the healthcare provider immediately
Answer: A. Reposition the mother to a left side-lying position
Explanation: Late decelerations indicate uteroplacental insufficiency, meaning the fetus is not getting enough oxygen. The first nursing intervention is to reposition the mother to a left side-lying position, as this improves blood flow to the placenta. Other interventions may follow.
- Option B (Administer oxygen) is appropriate, but positioning the patient takes priority.
- Option C (Increase IV fluids) may be necessary, as it improves perfusion to the uterus and placenta.
- Option D (Notify the healthcare provider) is essential if the interventions fail, but it is not the first action.
Question 3
A nurse is caring for a patient in active labor when the umbilical cord is seen protruding from the vaginal opening. What is the nurse’s priority action?
A. Place the patient in the Trendelenburg or knee-chest position
B. Gently push the umbilical cord back into the uterus
C. Notify the healthcare provider immediately
D. Apply a warm compress to the exposed cord
Answer: A.Place the patient in the Trendelenburg or knee-chest position
Explanation: A prolapsed umbilical cord occurs when the umbilical cord slips below the presenting part of the fetus, causing cord compression and decreased oxygen supply to the baby. The priority action is to position the mother in the Trendelenburg or knee-chest position to relieve pressure on the cord.
- Option B (Push the cord back) is incorrect and contraindicated, as it can cause more damage to the cord.
- Option C (Notify the provider) is essential, but it is not the first action. Immediate action is required to relieve pressure.
- Option D (Apply warm compress) is incorrect. The focus is on relieving pressure, not preserving cord temperature.