

Visual/Auditory

Preparing for the NCLEX PN® Exam requires a thorough understanding of the visual and auditory systems in child health, essential components of pediatric nursing care. Mastery of developmental milestones, common disorders, and their management is crucial. This knowledge aids in promoting optimal sensory development and addressing early signs of impairment.
Learning Objective
In studying “Visual/Auditory in Child Health” for the NCLEX PN® Exam, you should aim to understand the developmental aspects of vision and hearing in children, including normal growth patterns and common deviations. Learn to identify and manage common pediatric visual and auditory disorders such as strabismus, amblyopia, otitis media, and hearing impairments. Evaluate screening techniques and diagnostic tests used in early detection of these conditions. Additionally, explore the impact of sensory deficits on a child’s development and learning, and apply this knowledge to implement effective nursing interventions that support sensory health and overall developmental progress in pediatric patients.
Developmental Aspects of Vision and Hearing

The development of vision and hearing are complex processes that begin in utero and continue through early childhood, shaping how we perceive and interact with our environment. Understanding the developmental aspects of these senses helps in early detection of abnormalities and can guide interventions that may prevent long-term sensory impairments. Here’s an overview of how vision and hearing develop from infancy through childhood:
Development of Vision
- In Utero:
- Around the 20th week of gestation, fetuses can perceive light and by the 28th week, they can blink in response to bright lights.
- Birth to 2 Months:
- Newborns have limited vision, focusing best on objects about 8 to 10 inches away—the distance to a parent’s face during feeding.
- Infants prefer high-contrast patterns and can track slowly moving objects.
- 2 to 4 Months:
- Color vision develops, allowing infants to see a wide range of colors.
- Depth perception begins to develop as both eyes start to work together.
- 4 to 6 Months:
- Eye-hand coordination improves, enabling infants to reach for objects.
- Vision acuity sharpens, approaching that of an adult level.
- 6 Months to 1 Year:
- Babies begin to judge distances and throw objects with precision.
- They can recognize faces and differentiate between known and unknown individuals.
- Beyond 1 Year:
- By the age of two, visual acuity nearly reaches 20/20.
- Preschool years are critical for continuing visual development, with activities that can help improve visual discrimination and eye-hand coordination.
Development of Hearing
- In Utero:
- Hearing begins to develop around 16 weeks of gestation. By around 24 weeks, fetuses can respond to external sounds.
- Birth to 3 Months:
- Newborns can determine the direction of sounds and show preferences for certain types of sounds, such as their mother’s voice over others.
- 3 to 6 Months:
- Infants begin to associate sounds with their sources and start babbling, experimenting with producing sounds.
- 6 Months to 1 Year:
- Babies start to understand basic verbal commands and can recognize the names of common objects and family members.
- They enjoy games like “peek-a-boo” and “pat-a-cake” as they learn to associate sounds with actions.
- 1 Year and Beyond:
- Children refine their ability to locate sounds, recognize patterns in speech, and start to produce words and simple sentences.
- Hearing sensitivity and the ability to understand speech in noisy environments continue to develop throughout early childhood.
Common Visual Disorders in Children
Visual disorders in children can significantly affect their development and learning abilities. Early detection and treatment are crucial to prevent long-term visual impairment. Here are some common visual disorders that affect children:
1. Refractive Errors
- Myopia (Nearsightedness): Difficulty in seeing distant objects clearly. It’s common in school-age children and may worsen during growth spurts.
- Hyperopia (Farsightedness): Difficulty in seeing close objects clearly, which can lead to eye strain and headaches.
- Astigmatism: Caused by an irregularly shaped cornea or lens, leading to blurred vision at any distance.
2. Amblyopia (Lazy Eye)
- Occurs when the vision in one eye does not develop properly, making it weaker than the other. If untreated, amblyopia can lead to permanent vision loss in the affected eye. Common causes include significant refractive error in one eye, strabismus, or congenital cataracts.
3. Strabismus (Crossed Eyes)
- Misalignment of the eyes, where one or both eyes may turn inward, outward, upward, or downward. This condition can lead to amblyopia because the brain may start ignoring input from the misaligned eye to avoid double vision.
4. Congenital Cataracts
- Clouding of the eye’s lens present at birth or developing in early childhood. This condition can significantly impair vision and may require surgical removal of the cataract.
5. Retinopathy of Prematurity (ROP)
- A potentially blinding condition seen in premature infants. It involves abnormal growth of blood vessels in the retina and can lead to retinal detachment.
Common Auditory Disorders in Children
Auditory disorders in children can significantly impact language development, communication skills, and educational progress. Early detection and intervention are crucial to managing these conditions effectively. Here are some of the most common auditory disorders found in children:
1. Otitis Media (Middle Ear Infection)
- Description: Inflammation and infection of the middle ear, often accompanied by fluid accumulation. This condition is extremely common in children due to the shorter, more horizontal eustachian tubes.
- Symptoms: Ear pain, fever, and hearing difficulties.
- Treatment: Often resolves on its own, but severe cases may require antibiotics. Persistent fluid might necessitate surgical intervention, such as the placement of tympanostomy tubes (ear tubes).
2. Hearing Loss
- Conductive Hearing Loss: Typically caused by blockages or diseases affecting the outer or middle ear, such as otitis media, excessive earwax, or congenital malformations.
- Sensorineural Hearing Loss: Results from damage to the inner ear (cochlea) or auditory nerve. Causes include genetic factors, infections, exposure to loud noises, and complications at birth.
- Mixed Hearing Loss: A combination of conductive and sensorineural hearing loss.
3. Auditory Neuropathy Spectrum Disorder (ANSD)
- Description: A condition where sound enters the inner ear normally but the transmission of signals from the inner ear to the brain is impaired.
- Symptoms: Difficulty understanding speech clearly, especially in noisy environments.
- Treatment: Management strategies may include hearing aids, cochlear implants, or other forms of communication support like sign language or cued speech.
4. Auditory Processing Disorder (APD)
- Description: The brain’s inability to process sounds in the normal way.
- Symptoms: Difficulty understanding speech, especially in noisy environments, and problems with reading and spelling which are related to auditory skills.
- Treatment: Therapy strategies to improve auditory processing skills, modifications in classroom settings, and sometimes hearing aids.
5. Tinnitus
- Description: Hearing noises in the ears when no external sound is present. Although less common in children, it can occur and is often linked to sensorineural hearing loss.
- Symptoms: Buzzing, ringing, or whistling sounds in the ears.
- Treatment: Managing the underlying cause if known, sound therapy, and counseling to help mitigate the perception of tinnitus.
Nursing Care and Education
Nurses play a critical role in the management and education of children with visual and auditory disorders. Their responsibilities span from initial assessment and routine care to providing specific health education and supporting the child and their family. Here’s an overview of nursing care and education related to visual and auditory systems in child health:
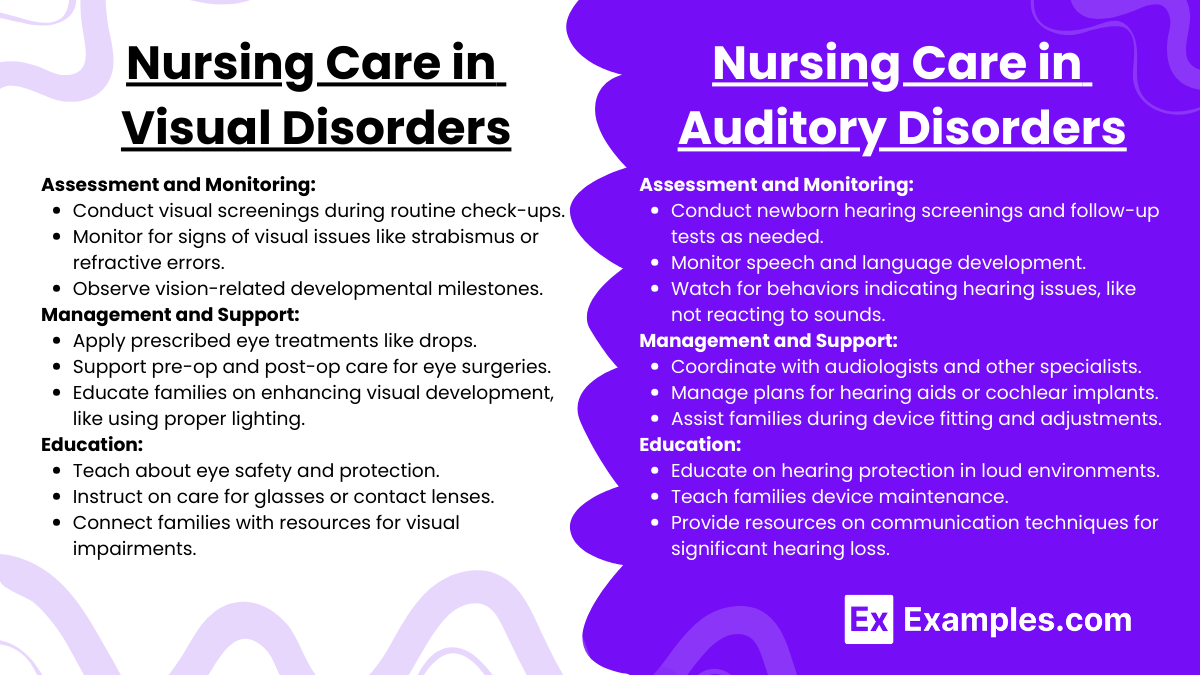
Nursing Care in Visual Disorders
- Assessment and Monitoring:
- Conducting routine visual screenings during well-child visits.
- Monitoring for signs of common visual disorders such as strabismus, amblyopia, or refractive errors.
- Observing developmental milestones related to vision.
- Management and Support:
- Administering prescribed treatments, such as eye drops for infections or allergies.
- Assisting in pre-operative and post-operative care for surgical procedures like correction of strabismus or removal of cataracts.
- Helping families understand and implement strategies for enhancing visual development, such as proper lighting for reading or using magnification tools.
- Education:
- Teaching families about the importance of eye protection and safety to prevent injuries.
- Instructing on the proper care and maintenance of corrective lenses or contact lenses.
- Providing resources and support for children with significant visual impairments, including connecting them with specialized services and educational programs.
Nursing Care in Auditory Disorders
- Assessment and Monitoring:
- Performing or facilitating newborn hearing screenings and subsequent audiometric testing if risks or problems are identified.
- Monitoring speech and language development milestones.
- Observing behaviors that might indicate hearing issues, such as not responding to sounds or delays in speech development.
- Management and Support:
- Coordinating care with audiologists, speech therapists, and otolaryngologists.
- Managing care plans for hearing aids, cochlear implants, or other assistive listening devices.
- Supporting children and families during the fitting and adjustment phases of hearing aids or cochlear implants.
- Education:
- Educating parents and children on the importance of hearing protection in noisy environments.
- Teaching families how to check and care for hearing devices.
- Providing information on communication techniques, such as sign language or cued speech, especially for families with children who have significant hearing loss.
Examples
Example 1: Managing Strabismus in a Toddler
- A toddler diagnosed with strabismus is referred for corrective treatment. The nurse educates the parents about the importance of patch therapy and potential surgical interventions if necessary. The nurse also coordinates follow-up appointments to assess improvements and ensure proper visual development.
Example 2: Treatment of Otitis Media
- A child with recurrent otitis media is treated with antibiotics. The nurse instructs the parents on the correct administration of medication and the importance of completing the full course. Advice on preventive measures such as avoiding smoke exposure and managing allergies is also provided to reduce future occurrences.
Example 3: Intervention for Congenital Cataracts
- A newborn is identified with congenital cataracts during a routine screening. The nurse assists in scheduling prompt surgical consultation and provides preoperative care instructions. Post-surgery, the nurse focuses on infection prevention, proper wound care, and scheduling regular visual assessments to monitor developmental milestones.
Example 4: Addressing Sensorineural Hearing Loss
- A school-aged child with sensorineural hearing loss is fitted with hearing aids. The nurse educates the child and family on how to use and care for the devices, ensuring comfort and optimal function. Information on assistive listening devices and communication strategies is also provided to support the child’s educational needs.
Example 5: Prevention of Noise-Induced Hearing Loss
- A teenager frequently exposed to loud music is counseled on the risks of noise-induced hearing loss. The nurse discusses the importance of hearing protection and safe listening practices, providing examples of appropriate ear protection devices and guidelines on how to monitor and limit exposure to loud noises.
Practice Questions
Question 1
Which intervention is most appropriate for a child diagnosed with amblyopia?
A. Patching the unaffected eye
B. Prescribing antibiotic eye drops
C. Surgical intervention on the affected eye
D. Use of corrective lenses only
Answer:
A. Patching the unaffected eye
Explanation:
Amblyopia, often called lazy eye, is commonly treated by patching the stronger, unaffected eye to force the weaker eye to work harder and develop better visual acuity. This treatment is most effective when started early and can significantly improve vision in the affected eye. Antibiotic eye drops (option B) are used for infections, not amblyopia, and surgical intervention (option C) may be considered in cases where other structural issues are present, but is not the primary treatment for amblyopia. Corrective lenses (option D) might be used but are usually supplemented by patching.
Question 2
Which screening test is used to detect hearing loss in newborns?
A. Tympanometry
B. Pure tone audiometry
C. Otoacoustic emissions (OAE) testing
D. Visual reinforcement audiometry
Answer:
C. Otoacoustic emissions (OAE) testing
Explanation:
Otoacoustic emissions (OAE) testing is commonly used to screen for hearing loss in newborns. This test measures sound waves produced in the inner ear, which disappear or diminish in the presence of hearing loss. It is effective, non-invasive, and can be performed while the infant is asleep. Tympanometry (option A) is used to evaluate middle ear function, not hearing sensitivity, and pure tone audiometry (option B) and visual reinforcement audiometry (option D) are used in older children who can respond to auditory cues.
Question 3
What is the primary cause of conductive hearing loss in children?
A. Noise exposure
B. Otitis media
C. Genetic disorders
D. Neurological conditions
Answer:
B. Otitis media
Explanation:
Otitis media, or middle ear infection, is the most common cause of conductive hearing loss in children. It occurs when fluid accumulates in the middle ear, typically due to infection, which can block the transmission of sound to the inner ear. Managing otitis media effectively can prevent or minimize associated hearing loss. Noise exposure (option A) mainly causes sensorineural hearing loss, while genetic disorders (option C) and neurological conditions (option D) are less likely to cause conductive hearing loss directly.